
Research has shown up to 65% of all shoulder pain is related to shoulder impingement syndrome. 4 What does this mean and how can this condition be prevented?
Shoulder impingement syndrome is a chronic condition that progresses and develops over time. It is caused by the compression and pinching of muscle, nervous tissue or bursa between the bony structures of the shoulder, and leads to irritation and inflammation of the soft tissue surrounding the shoulder.1,2,3,4,5, Friction and pressure may eventually produce micro-tears within the tissues. 3 Needless to say, this condition can produce a fair amount of pain and discomfort.
![]()
Subacromial impingement syndrome is very common in athletes such as swimmers who perform a lot of overhead motions; however, this condition is not limited to athletes, it is also very common in the general population.
The causes of impingement include: structural variations, functional instability or a combination of structural and functional instabilities. 2 ,5 Structural variations include oddly shaped bones or bony growths and inflamed tissues. 5 In contrast, functional instability refers to muscular imbalances, which can encourage poor posture and increase the likelihood of shoulder injury. To fully understand the nature of this condition let’s review the anatomy of the shoulder.
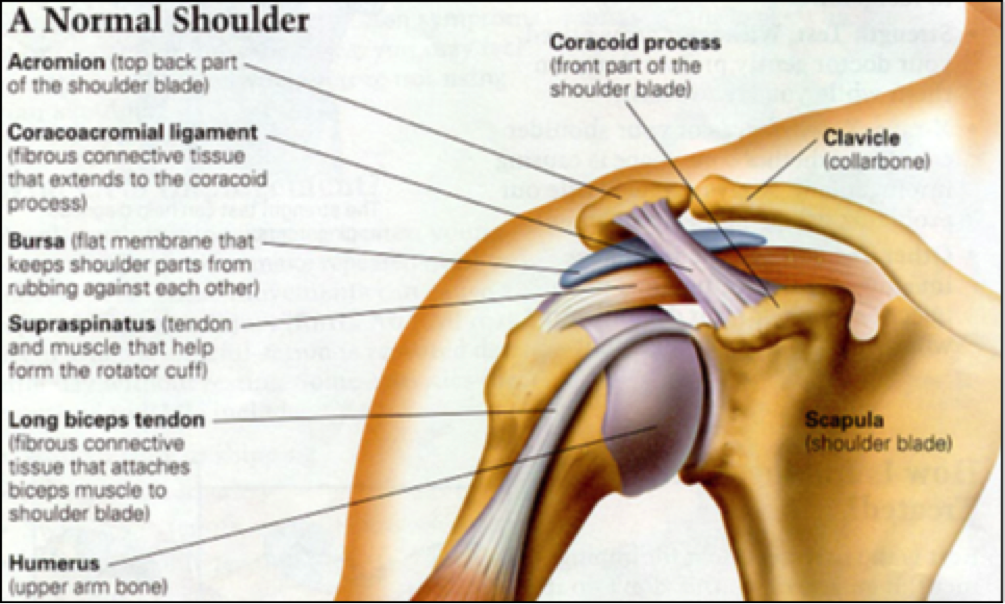
ANATOMY OF THE SHOULDER
The shoulder is comprised of 3 interconnected bones: the humerus, collar bone (also known as the clavicle), and the shoulder blade (also known as the scapula). Together they form the 4 joints of the shoulder:
Glenohumeral joint – between the humerus and the shoulder blade
Acromioclavicular joint- between the acromion process of the shoulder blade and the collar bone
Sternoclavicular joint – between the sternum and collar bone Scapulothoracic joint- between the shoulder blade and rib cage
Subacromial space (**space between the head of the humerus and the acromion process of the shoulder blade where soft tissues of the shoulder are compressed**)
These joints work together to give the shoulder great mobility; however, without proper balance of the musculature which allows movement at these joints, the shoulder can become unstable and an individual may become more prone to developing conditions such as shoulder impingement.
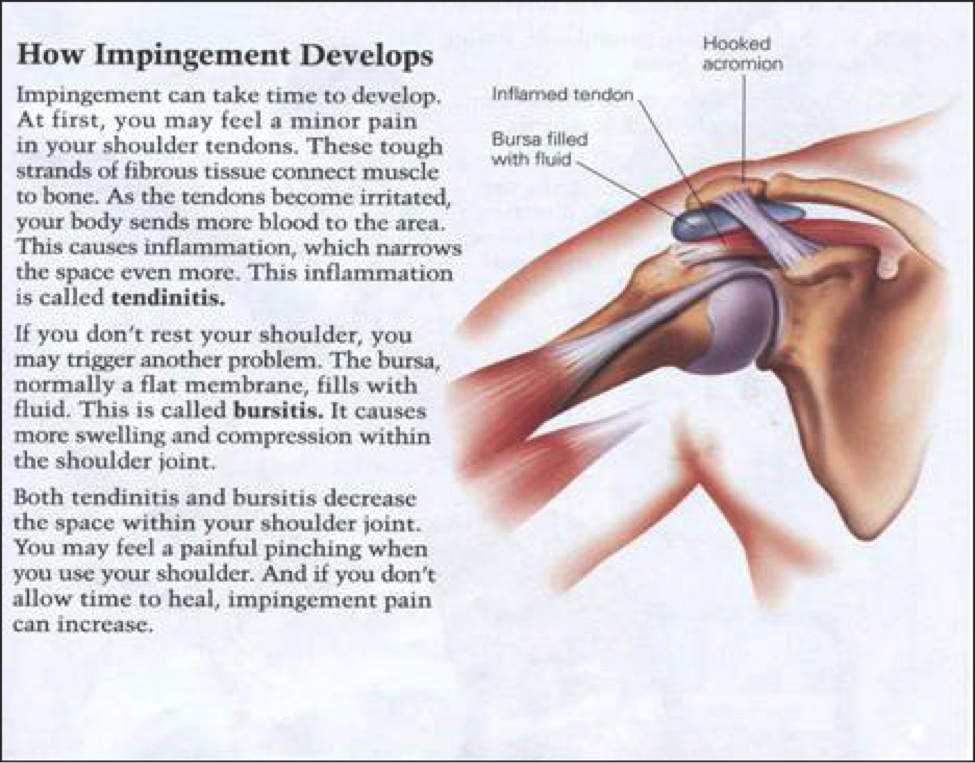
HOW SUBACROMIAL IMPINGEMENT DEVELOPS
Many activities in our daily lives involve elevating our arms outwards above our heads. This simple motion involves all 4 shoulder joints. The humerus rotates in its socket, the shoulder blade rotates along the ribcage and the collarbone elevates to produce this overhead motion. It is with this outwards elevation of the arm that the head of the humerus and acromion process of the shoulder blade gradually move closer to one another, narrowing the subacromial space along which 3 major structures run.
These structures include: 2, 4, 5
– Biceps long head tendon
– Supraspinatus tendon
– Subacromial bursa
The combination of inflamed tissue, bony growths or altered posture with the natural narrowing of subacromial space during overhead movements is enough to cause the compression of one or more of the above structures.
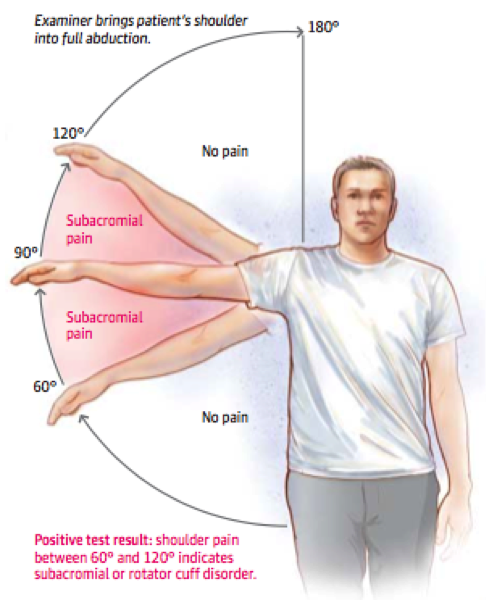
PATTERNS & SIGNS SUBACROMIAL IMPINGEMENT SYNDROME
There are several common patterns exhibited by individuals with subacromial impingement syndrome.
1) Painful range of motion termed the “painful arc” occurs between 60-120 degrees of outward elevation.1 Below 60 degrees and above 120 degrees individuals are generally able to move their shoulders without the presence of pain.
2) The structure which is most commonly compressed within the subacromial space is the supraspinatus tendon since it is “most likely to contact the acromion”.5
3) Individuals with subacromial impingement syndrome due to functional instability will often have over development or tightness within some muscles and weakness in other regions. A common pattern of muscle imbalance is weakness within the middle and lower fibers of the trapezius muscle, posterior deltoid, serratus anterior and rotator cuff muscles with a profound tightness or overdevelopment of the pectoralis major, upper trapezius fibers, and levator scapulae.
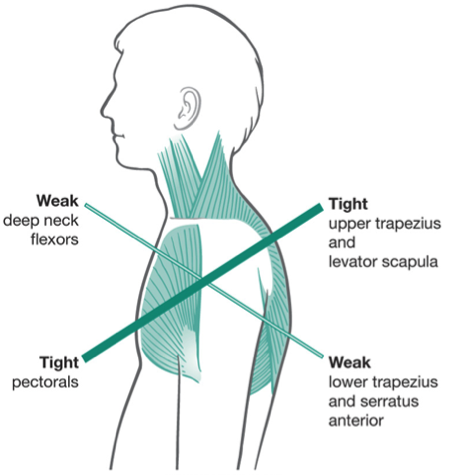
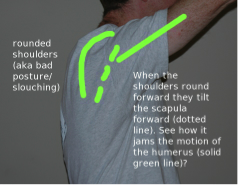
The combination of weakness and tightness within these muscles shifts the shoulder blade slightly upwards and forward and rotates the shoulders forward and inwards creating rounded shoulders and a slouched posture.

TREATMENT, TIPS & EXERCISES
Treatment of subacromial shoulder impingement syndrome is dependent on the cause of the impingement itself. As discussed earlier, impingement can be as result of structural variations in the body such as bony growths. In such cases, treatment options may include surgical procedures, but subacromial shoulder impingement due to functional instability can be effectively managed with physiotherapy in the form of manual treatments and therapeutic exercise. 5
Regardless of the cause of shoulder impingement, an effective treatment is the use of ice. Icing constricts blood vessels reducing the blood flow to the affected area thereby helping to reduce inflammation and reduce pain. 2
In the treatment of subacromial impingement syndrome caused by functional instability due to muscular imbalance, posture is a major consideration. We live in a society where much of our time is spent commuting in our vehicles, sitting behind our desks, or burying our noses in textbooks. It is not surprising that as a result, our posture suffers.
Tips for improving your posture at work and on the go:
1) Remind yourself with a sticky note at your workstation to sit tall and with good posture.
2) Use a lumbar support pillow on your office chair.
3) Get in your vehicle, sit tall with good posture and adjust your rearview mirror. While driving if you can no longer see in your rearview mirror this will be a clear reminder you are slouching and should straighten up.

Helpful exercises to help alleviate impingement & counteract poor posture:
In the initial stages of treatment, exercises which involve motion within the patients “painful arc” should be avoided. Focus should be placed on stretching tight musculature and strengthening weak musculature. 2
Stretches should include pectoral stretches and should be performed in sets of 5 2-3 times per day. All stretches should be held for 10-15 seconds.

For resistance exercises, a general guideline is to complete 3 sets of 10 repetitions of each exercise once daily. Some beneficial exercises include:
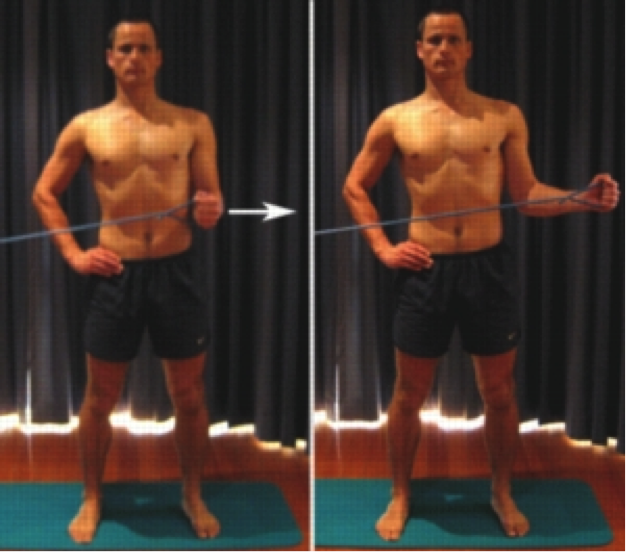
Shoulder External Rotation with Thera-tubing: This exercise will target the muscles of the rotator cuff.
Rows with Thera-tubing: This exercise will focus on strengthening the middle and lower fibers of the trapezius muscle. During this exercise, your focus should be placed on drawing the shoulder blades together while keeping the shoulders relaxed and avoiding a shrugging motion.
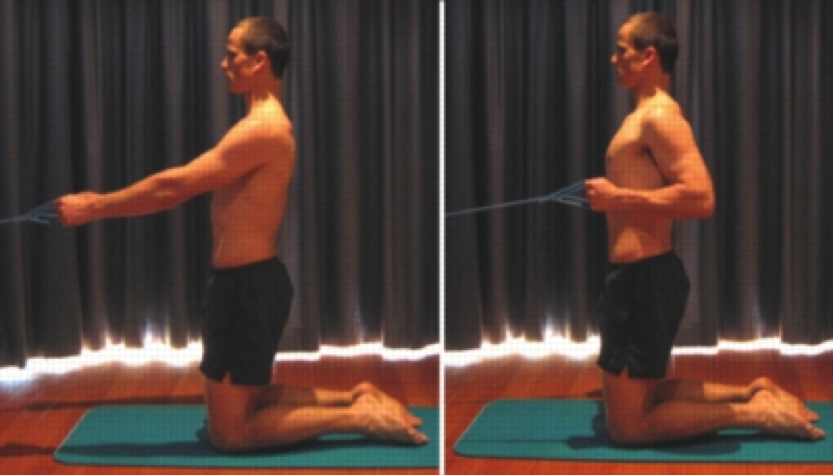
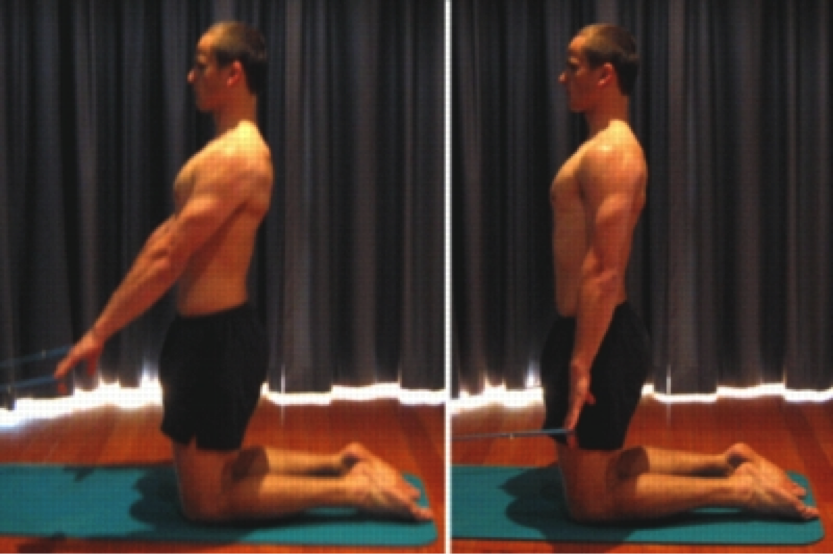
Shoulder Extension with Thera-tubing: During this exercise, your focus should be placed on drawing the shoulder blades down and inward while keeping the shoulders relaxed and avoiding a shrugging motion.
References
1 Braun, C., Bularcyzk, M., Heintsch, J., & Hanchard, N.C.A. (2013). Manual therapy and exercises for shoulder impingement revisited. Physical Therapy Reviews 18(4). 263-284.
2 Escamilla, R. F., Hooks, T.R. & Wilk, K.E. (2014).Optimal management of shoulder impingement syndrome. Open Access Journal of Sports Medicine, 5(1). 13-24.
3 Fontaine, M. (2014). Shoulder Impingement: The keys to dealing with swimmers ! shoulder. American Chiropractic Association News, 20-21.
4 Norris, C. (2014). Shoulder Impingement. SportEX dynamics, 42(1). 21-28.
5 Page, P. (2011). Shoulder muscle imbalance and subacromial impingement syndrome in overhead athletes. International Journal of Sports Physical Therapy, 6(1). 51-58.
Figure References
Figure 1. Retrieved from http://therotater.com/blog/wp-content/uploads/2011/02/ Shoulder-Impingement-101.png
Figure 2. Retrieved from http://www.ortho-md.com/images/proceduresImg/ SHOULDER1.jpg
Figure 3. Retrieved from https://s-media-cache-ak0.pinimg.com/originals/c4/65/a7/ c465a7538e3fb5ac78ce63bd39401891.jpg
Figure 4. Retrieved from https://jcphysiotherapy.files.wordpress.com/2015/02/screen- shot-2014-05-07-at-2-27-45-pm.png
Figure 5. Retrieved from http://saycoperformance.com/blog/wp-content/uploads/ 2011/05/upper-crossed-syndrome2.png
Figure 6 & 7. Retrieved from http://athletestreatingathletes.com/wp/wp-content/uploads/ 2013/01/roundedshldr1.jpg
Figure 8. http://www.mindinmotionkc.com/wp-content/uploads/2014/04/you-have-bad- posture-candy-cane.jpg
Figure 9. Retrieved from http://www.bloomtofit.com/wp-content/uploads/2012/01/ pectorialis-stretch.jpg
Figure 10, 11, 12. Retrieved from http://www.physioadvisor.com.au/8120750/upper- back-exercises-upper-back-strengthening-ex.htm